1601006175 hall ticket no. Long case
1601006175 long case
This is an online e logbook to discuss our patients deidentified health data shared after taking his / guardian’s signed informed consent.
Here we discuss our individual patient problems through a series of inputs from available global online community experts with an aim to solve those patients clinical problems with collective current best evidence based inputs.
This e log also reflects my patient centre’s online portfolio and valuable inputs on comment box is welcomed.
A 45 year old male patient who’s a farmer by occupation came to OPD with
Chief complaints :
Shortness of breath since 2 years
Decreased urine output since 2 years
Pedal edema since 2 years
History of present illness :
Patient was apparently asymptomatic 2 years ago then he developed ,shortness of breath which was insidious in onset gradually progressive, which progressed to the present stage (from class 2 progressedto class 4 ) there were ,no relieving factors. He also had bilateral pedal edema since 2 years which was also insidious in onset and gradually progressive , presently he is having grade 4 pitting type of bilateral pedal edema till below knee ,which did not relieved on rest or medication. There was also decrease in urine output since 2 years, he passed urine daily once which was scanty in amount , there was n burning micturition or dysuria.
Along with these symptoms he also had loin pain which was continuous & not radiating type . Due to his illness he has not been working since 2 years. All these symptoms persisted even after his regular sessions of dialysis ( twice weekly ) and this time they have become even more serious and was admitted in the hospital.
Past history:
The patient is a known case of hypertension since 12 years for which he is taking medication regularly in since 2 years before which he was taking irregular medication.
No history of
Diabetes mellitus, tuberculosis , bronchial asthma, epilepsy
Family history: not significant
Personal history :
diet : mixed
Appetite : reduced
Bowel movemets: regular
Bladder movements : irregular
Sleep : decreased
Addictions : nil
Drug history:
Before 2 years he was taking irregular medication- telvas 40 mg OD
Presently he is using Nicardipine prolonged release tablets 20 mg , metoprolol succinate extended release 25mg .
General examination:
The patient was conscious, coherent & cooperative , ill built & undernourished.
There were signs of pallor

bilateral pedal edema


There were no signs of icterus , clubbing , cyanosis , koilonychia & lymphadenopathy
Vitals :
Temperature: afebrile
Pulse : 64 bpm regular ,normal volume
Blood pressure: 120/80
Respiratory rate: 21 cpm abdominothoracic
Systemic examination:
Abdominal examination:
Inspection : localised asymmetrical fullness in the left lumbar region
Umbilicus central in location and slightly retracted.


Abdomen was moving accordingly with respiration.
No visible pulsation , no visible gastric peristalsis, no visible scars and sinuses
Palpation:
No local rise of temperature. No organomegaly.
Percussion :
Dull note in the flanks & tympanic note in the centre ( around the umbilicus)
Auscultation:
Normal bowel sounds were heard.
Respiratory examination:
Inspection:
Trachea is central in position. Shape of the chest elliptical . Bilaterally equal chest movements with respiration. There was supra scapular hollowness .
No scars and sinuses
Palpation:
No local rise of temperature. All the inspectory findings were confirmed
Trachea is in central position.
Apex beat displaced laterally.
Tactile vocal fremtus was normal
Chest expansion was normal.
Percussion:
On direct percussion of clavicle-
2nd to 5th intercostalspace on right side & 2nd to 6 th intercostal space on the left side - resonant note
Auscutation: normal vesicular breath sounds heard in supra mammary & infra mammary areas on both right and left sides.
Cardiac examination:
there was no precordial bulge on inspection . S1 & s2 were heard in mitral , tricuspid, aortic & pulmonary areas .no added sounds were heard.
Cns examination: no facial asymmetry , all the reflexes were normal
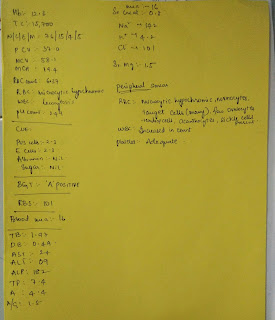
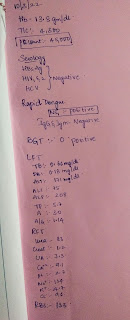
INVESTIGATIONS :






ECG

X-ray


This is an online e logbook to discuss our patients deidentified health data shared after taking his / guardian’s signed informed consent.
Here we discuss our individual patient problems through a series of inputs from available global online community experts with an aim to solve those patients clinical problems with collective current best evidence based inputs.
This e log also reflects my patient centre’s online portfolio and valuable inputs on comment box is welcomed.
A 45 year old male patient who’s a farmer by occupation came to OPD with
Chief complaints :
Shortness of breath since 2 years
Decreased urine output since 2 years
Pedal edema since 2 years
History of present illness :
Patient was apparently asymptomatic 2 years ago then he developed ,shortness of breath which was insidious in onset gradually progressive, which progressed to the present stage (from class 2 progressedto class 4 ) there were ,no relieving factors. He also had bilateral pedal edema since 2 years which was also insidious in onset and gradually progressive , presently he is having grade 4 pitting type of bilateral pedal edema till below knee ,which did not relieved on rest or medication. There was also decrease in urine output since 2 years, he passed urine daily once which was scanty in amount , there was n burning micturition or dysuria.
Along with these symptoms he also had loin pain which was continuous & not radiating type . Due to his illness he has not been working since 2 years. All these symptoms persisted even after his regular sessions of dialysis ( twice weekly ) and this time they have become even more serious and was admitted in the hospital.
Past history:
The patient is a known case of hypertension since 12 years for which he is taking medication regularly in since 2 years before which he was taking irregular medication.
No history of
Diabetes mellitus, tuberculosis , bronchial asthma, epilepsy
Family history: not significant
Personal history :
diet : mixed
Appetite : reduced
Bowel movemets: regular
Bladder movements : irregular
Sleep : decreased
Addictions : nil
Drug history:
Before 2 years he was taking irregular medication- telvas 40 mg OD
Presently he is using Nicardipine prolonged release tablets 20 mg , metoprolol succinate extended release 25mg .
General examination:
The patient was conscious, coherent & cooperative , ill built & undernourished.
There were signs of pallor

bilateral pedal edema


There were no signs of icterus , clubbing , cyanosis , koilonychia & lymphadenopathy
Vitals :
Temperature: afebrile
Pulse : 64 bpm regular ,normal volume
Blood pressure: 120/80
Respiratory rate: 21 cpm abdominothoracic
Systemic examination:
Abdominal examination:
Inspection : localised asymmetrical fullness in the left lumbar region
Umbilicus central in location and slightly retracted.


Abdomen was moving accordingly with respiration.
No visible pulsation , no visible gastric peristalsis, no visible scars and sinuses
Palpation:
No local rise of temperature. No organomegaly.
Percussion :
Dull note in the flanks & tympanic note in the centre ( around the umbilicus)
Auscultation:
Normal bowel sounds were heard.
Respiratory examination:
Inspection:
Trachea is central in position. Shape of the chest elliptical . Bilaterally equal chest movements with respiration. There was supra scapular hollowness .
No scars and sinuses
Palpation:
No local rise of temperature. All the inspectory findings were confirmed
Trachea is in central position.
Apex beat displaced laterally.
Tactile vocal fremtus was normal
Chest expansion was normal.
Percussion:
On direct percussion of clavicle-
2nd to 5th intercostalspace on right side & 2nd to 6 th intercostal space on the left side - resonant note
Auscutation: normal vesicular breath sounds heard in supra mammary & infra mammary areas on both right and left sides.
Cardiac examination:
there was no precordial bulge on inspection . S1 & s2 were heard in mitral , tricuspid, aortic & pulmonary areas .no added sounds were heard.
Cns examination: no facial asymmetry , all the reflexes were normal
INVESTIGATIONS :






ECG

X-ray

Provisional diagnosis : chronic kidney disease with maintenance dialysis.
Drugs used -




Comments
Post a Comment